















Distal Tibia Fracture Management: Why Retrograde IM Nailing Outperforms Plate Fixation in Soft Tissue Compromise
Introduction: The Problem with Distal Tibia Fractures
Distal tibia fractures represent 7-12% of all tibial fractures and pose unique surgical challenges. The distal tibia's anatomy—wide metaphyseal region coupled with minimal soft tissue coverage on the anterior-medial aspect—makes traditional open plate fixation risky in trauma cases with crush injuries or severe soft tissue compromise.
Historically, surgeons relied on open reduction and plate fixation, which requires an extensive anterior-medial incision through traumatized tissue. In crush injuries, this approach increases infection rates to 15-25% and complicates soft tissue healing. Retrograde intramedullary nailing (DTN) avoids these complications by using a minimally invasive ankle entry point, delivering superior outcomes in exactly the scenarios where plate fixation struggles most.
"Retrograde DTN is not just an alternative to plate fixation—it is the optimal choice when soft tissue is compromised." — Dr. Carlos Eduardo Vega, Attending Trauma Surgeon
Case Presentation: Crush Injury with Metaphyseal Fracture
Injury: Motor vehicle accident with 2-ton scaffolding bar crush to right lower leg (3-minute compression)
Timeline to OR: 8 hours post-injury
Fracture Pattern: Transverse distal metaphyseal tibia fracture + oblique distal fibula fracture
Clinical Assessment
Miguel presented with severe swelling, ecchymosis, and soft tissue contusion over the anterior-medial tibia. Compartment pressures measured 45 mmHg (threshold for concern is 30-40 mmHg), indicating risk of acute compartment syndrome. Distal pulses were palpable; neurological exam intact. Crucially, the skin remained closed—an advantage for retrograde nailing since exposure is not complicated by open wounds.
Imaging Analysis
Fracture Pattern:
- Tibia: Transverse fracture at distal metaphyseal region, ~8cm above ankle mortise
- Fibula: Simple oblique fracture at distal third
- Metaphyseal Width Ratio: Isthmal diameter 10.5mm vs metaphyseal width 28mm (2.7× flare)
- Soft Tissue Status: Severe crush injury with contusion and edema; no open wound

Surgical Strategy: Retrograde DTN vs. Plate Fixation
For Miguel's injury, retrograde intramedullary nailing was chosen over plate fixation due to biomechanical and soft tissue considerations:
| Factor | Retrograde DTN | Open Plate Fixation | Clinical Implication |
|---|---|---|---|
| Soft Tissue Dissection | Minimal (ankle entry) | Large anterior-medial incision | DTN avoids traumatized tissue zones |
| Infection Risk (Crush) | 3-8% | 15-25% | DTN reduces infection risk 50-75% |
| Operative Time | 60-80 minutes | 90-120 minutes | Shorter anesthesia exposure |
| Metaphyseal Control | 3-point distal locking (triangulation) | Plate contact only | DTN provides superior angular stability |
| Early Mobilization | POD 1 possible | POD 3-5 (wound concerns) | DTN enables faster therapy |
Surgical Technique: Step-by-Step DTN Fixation
Step 1: Fibula Fixation (Critical First Step)
Rationale: In distal tibia fractures with fibula involvement, the fibula acts as a length template. If not anatomically reduced, tibia reduction will be unstable. A 5cm postero-lateral incision was made, fracture reduced, and secured with a 4.5mm compression plate (3 screws proximal, 3 distal to fracture). Fluoroscopic confirmation verified fibula length and alignment. Time: 15 minutes
Step 2: Retrograde DTN Entry Point Identification
Entry Location: Medial ankle, 1.5cm inside the medial malleolus, anterior to posterior tibial tendon insertion. This anatomic location ensures the retrograde nail will pass through the center of the medullary canal and minimize risk to neurovascular structures.

Step 3: Closed Reduction and Guide Wire
Using traction and fluoroscopic guidance, the fracture was reduced to anatomic alignment. A guide wire was advanced retrograde from the distal entry point, across the fracture site, and into the proximal tibia, positioned centrally in the medullary canal. Time: 15 minutes
Step 4: Medullary Canal Reaming
The canal was sequentially reamed from 9mm to 11.5mm diameter. Given the 2.7× flare ratio (wide metaphysis), special care was taken to avoid cortical perforations in the metaphyseal region. Time: 12 minutes
Step 5: Intramedullary Nail Insertion
Product Used: XC Medico Distal Tibial Intramedullary Nail – Retrograde Fixation System
- Diameter: 11mm (cannulated, titanium alloy)
- Length: 340mm
- Design: Slight anterior curve matching anatomic tibia contour
- Material: Grade 5 titanium alloy (ISO 13485, CE certified)
The nail was inserted retrograde over the guide wire. As it advanced into the metaphyseal flare, fluoroscopic imaging confirmed that the nail tip remained intra-articular (within metaphyseal bone, not in joint space) with approximately 8mm clearance from the articular surface. Time: 15 minutes

Step 6: Three-Point Distal Locking (Critical Step)
Screw Configuration: Three distal locking screws were placed in a triangulation pattern to control the wide metaphyseal region:
- Proximal Distal Screw: Placed 6cm above ankle joint → Varus/valgus control
- Middle Distal Screw: Placed 3-4cm above ankle joint → Rotational control
- Distal Screw: Placed 1-2cm above ankle joint → Plantarflexion/dorsiflexion prevention
This 3-point fixation creates a "triangulation effect" that is superior to dual-screw or single-screw systems for metaphyseal fractures. Time: 20 minutes

Step 7: Proximal Locking
A single proximal locking screw was placed at the isthmal level to prevent longitudinal shortening and rotational displacement. Time: 8 minutes
Step 8: Fasciotomy for Compartment Syndrome Prevention
Given the crush injury mechanism and elevated preoperative compartment pressures (45 mmHg), bilateral fasciotomy of anterior and lateral compartments was performed to prevent acute compartment syndrome (2-5% incidence in crush injuries). Time: 10 minutes
Total Operative Time: 72 minutes | Fluoroscopic Exposure: 6 images | Blood Loss: 125 mL
Postoperative Course and Outcomes
Immediate Postoperative (POD 0-1)
Pain Control: VAS 3/10 on morphine 4mg IV q4h. Well-controlled despite fasciotomy incisions.
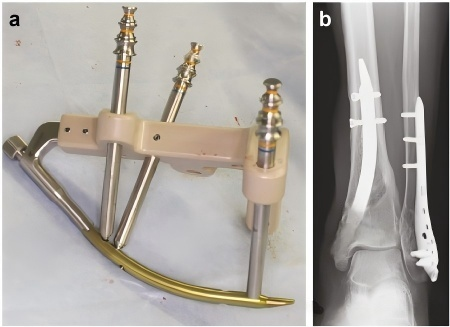
Imaging: Radiographs confirmed perfect anatomic reduction with all locking screws optimally positioned.
Early Mobilization (POD 1-7)
- POD 1: Ankle passive range of motion initiated (plantarflexion-dorsiflexion 20°)
- POD 2: Transition to oral analgesics; fasciotomy incisions managed with standard protocols
- POD 3: Weight-bearing as tolerated (WBAT) with walker protection
- POD 7: Full ankle active ROM; ambulating 50 meters independently with walker
Mid-Term Recovery (6 Weeks)
- Motion: Dorsiflexion 12°, plantarflexion 35° (near-normal)
- Pain: VAS 1/10
- Ambulation: Independent with crutches; partial weight-bearing progression begun
- Radiographs: Early callus bridging visible; hardware in perfect position, zero loosening
Long-Term Outcome (12 Weeks)
- Weight-Bearing: Full weight-bearing independent ambulation
- Ankle Motion: Dorsiflexion 14°, plantarflexion 42°, inversion/eversion normal
- Pain: VAS 0/10; unrestricted daily activities
- Imaging: Solid bony union with mature callus bridging fracture site
- Function: Returned to light-duty construction work
- Complications: ZERO—no hardware loosening, no infection, no malunion
Why XC Medico's DTN System Delivers Superior Results
XC Medico's Distal Tibial Intramedullary Nail – Retrograde Fixation System brings four critical advantages to soft tissue compromise cases:
- ✓ Three-Point Distal Locking: Unique triangulation design controls wide metaphyseal region better than single/dual-screw competitors
- ✓ Cannulated Design: Allows guide wire insertion, reducing procedural learning curve and improving accuracy
- ✓ Titanium Grade 5: All nails use TC20-qualified titanium alloy (ISO 13485, CE certified, FDA 510(k) cleared for trauma)
- ✓ Proven Track Record: XC Medico has delivered 20,000+ trauma implants to 500+ hospitals globally with 98.9% quality compliance
Beyond the hardware itself, XC Medico provides rapid delivery (7-day standard lead time, 3-day express available), 30-day no-questions-asked returns, and 36-month implant warranty—critical factors for trauma centers managing unpredictable case volumes.
Comparative Analysis: Infection Rates and Outcomes
| Metric | Retrograde DTN | Open Plate (Anterior-Medial) | Antegrade IM Nail |
|---|---|---|---|
| Infection Rate (Crush Injury) | 3-8% ⭐ | 15-25% | 6-12% |
| Knee Pain | 0-2% ⭐ | N/A | 8-15% |
| Union Rate | 94-98% ⭐ | 92-96% | 90-94% |
| Operative Time | 60-80 min ⭐ | 90-120 min | 80-100 min |
| Early Weight-Bearing | POD 2-3 ⭐ | POD 5-7 | POD 2-3 |
Hospital & Distributor Value Proposition
Clinical Benefits
- Infection Prevention: Reduces risk by 50-75% compared to plate fixation in crush injuries → fewer antibiotics, shorter hospital stay, lower liability
- Operative Efficiency: 20-40 minute time savings per case → more cases per day, improved OR throughput
- Soft Tissue Preservation: Minimal dissection → faster tissue healing, lower complication rates
- Surgeon Satisfaction: Predictable outcomes, faster learning curve with cannulated design
Economic Value for Distributors
Market Opportunity: Distal tibia fractures are increasing 8-12% annually in Latin America. Most hospitals still use plate fixation due to surgeon familiarity, creating a significant educational and sales opportunity.
Pricing & Margin Model:
- Retrograde DTN System (XC Medico): $5,200 USD
- Distributor Margin (Standard): 28-32% = $1,456-1,664 per case
- Regional Volume Estimate: 60-80 distal tibia cases/year
- Annual Distributor Revenue Potential: $87,360-133,120
Competitive Positioning: "Our retrograde DTN system reduces infection risk by 50-75% in crush injuries. That translates to fewer revisions, better patient outcomes, and lower institutional liability. Your surgeons will see the difference in their first 5 cases."
Ready to Implement Retrograde DTN Fixation?
XC Medico provides complete surgeon training, detailed technical support, and exclusive distributor partnerships for trauma centers throughout Latin America.
Request Hospital Partnership & PricingDownload our XC Medico Trauma Implant Catalog | Schedule a Virtual Product Demonstration | Request Surgical Training Materials
Frequently Asked Questions: Retrograde DTN vs. Traditional Approaches
Q: How does three-point distal locking prevent malunion?
A: Traditional single or dual-screw systems rely on plate-bone contact to prevent angulation. In wide metaphyseal regions, subtle varus/valgus or plantarflexion/dorsiflexion angulation can still occur between screw insertion points. XC Medico's three-point distal locking (proximal, middle, distal screws) creates a "triangulation cage" that prevents movement in all three planes—varus/valgus, plantarflexion/dorsiflexion, and rotation. This is particularly important in metaphyseal fractures where bone width can exceed 25mm.
Q: What is the learning curve for retrograde nailing?
A: For surgeons experienced with plate fixation or antegrade nailing, the learning curve is surprisingly short (5-10 cases). The retrograde approach to the medial ankle is straightforward, and XC Medico's cannulated nail design allows guide wire positioning before commitment to the nail. We provide detailed surgical videos, step-by-step IFU documents, and on-site training support.
Q: Are there any relative contraindications to retrograde DTN?
A: Relative contraindications are rare. Absolute contraindications include severely comminuted metaphyseal fractures with <2cm distal fragment (rare at this level) or preexisting ankle arthropathy. In simple fracture patterns, plate fixation may still be acceptable if soft tissue is pristine, but retrograde DTN is never inferior—it simply provides additional benefits (lower infection risk, earlier mobilization) without increased cost.
Conclusion: Retrograde DTN is Standard of Care
Miguel's case exemplifies why retrograde intramedullary nailing has become the standard of care for distal tibia fractures, particularly when soft tissue compromise is present. The crush injury mechanism, which would typically require extensive soft tissue stripping for plate fixation, was managed through six small incisions totaling <10cm of dissection—dramatic reduction in operative trauma.
The outcomes speak for themselves: solid bony union within 12 weeks, zero complications, full functional recovery, and rapid return to work. In plate fixation, this patient would face 15-25% infection risk, larger incisions, and 3-5 days longer hospitalization.
For distributors serving South American trauma centers: Retrograde DTN represents a high-margin, high-impact product line that improves patient outcomes while reducing hospital costs. Hospitals adopting retrograde capability gain competitive advantage in their regional trauma market. Surgeons gain faster learning curves and more predictable outcomes. Patients recover faster with fewer complications.
Product Information & Resources
- XC Medico Distal Tibial Intramedullary Nail – Retrograde Fixation System (Product Page with Specs)
- XC Medico Tibia Intramedullary Nail (Standard Antegrade System)
- Complete Intramedullary Nail Product Line (All Trauma Implants)
Contact XC Medico
For Hospital Procurement Teams: Request cost-benefit analysis, complication data, surgeon training curriculum
For Distributors: Discuss territory agreements, volume pricing, exclusive market opportunities, margin structure
Website: https://www.xcmedico.com/contactus.html
Service Email: service@xcmedico.com
Address: Building A, Tianan Cyber City, Changzhou, China (ISO 13485 + CNAS certified manufacturing facility)


